Using HDsEMG to Uncover Neuromuscular Biomarkers in Children with Developmental Coordination Disorder (DCD)
How motor unit decomposition reveals neuromuscular patterns associated with motor control deficits
Key Takeaways
1
Developmental Coordination Disorder affects about 1/20 children and is characterized by difficulties in performing activities of daily living due to deficits in motor control. However, little is currently known about the neuromuscular patterns associated with DCD.
2
Using HDsEMG, researchers have been able to record motor unit data to better understand the differences in neuromuscular activity between typically developing (TD) children and children with DCD.
3
Results indicate that children with DCD have more fixed motor unit firing strategies, which may explain why they struggle to adopt new movement patterns.
What is Developmental Coordination Disorder?
In a typical classroom, at least one child will have DCD – a developmental disorder characterized by difficulties in performing activities of daily living due to deficits in movement control. Children with DCD may appear uncoordinated or overly clumsy; they tend to struggle when performing age-appropriate motor tasks, which can cause frustration and impact their social lives. This disorder affects around 5% of children, yet it is often overlooked and considered a symptom of other disorders.
Children with DCD struggle with:
Everyday tasks: Tying their shoelaces, using a fork and knife, and opening bottles
Sports and social activities: Catching and throwing in PE class, participating in organized sports, and playing musical instruments.
General balance: Tripping and falling regularly
A Paradigm Shift in the Understanding of DCD
Until recently, DCD was widely misunderstood and often thought of as a subset of Attention-Deficit/Hyperactivity Disorder (ADHD). Although children with DCD frequently also experience ADHD, these two conditions are fundamentally different, and their underlying mechanisms must be understood independently.
Traditional approaches for managing DCD have largely focused on addressing specific motor control deficits through occupational and physical therapy. While these approaches can help children make short-term, task-specific performance improvements, they often fail to address the persistent challenges of motor control and daily functioning that have the greatest impact on children with DCD.
Crucially, it is not known how these therapies impact the deeper neuromuscular mechanisms that contribute to the condition, leaving fundamental questions about their efficacy unanswered. More broadly, this lack of understanding makes classification and management of DCD a major challenge.
Shifting the focus to the neuromuscular underpinnings of DCD represents a transformative change in how the condition is understood and managed. For instance, do existing therapies induce meaningful changes at the neuromuscular level, or are they merely equipping children with strategies to perform isolated tasks? Are task-specific interventions limiting in scope, and could therapies targeting neuromuscular development lead to broader, more sustained improvements? These are pivotal questions driving contemporary research.
Dr. Maaike Esselaar
Manchester Metropolitan University
Using HDsEMG to Identify Neuromuscular Markers in Children with DCD
Research by Dr. Maaike Esselaar and her team at Manchester Metropolitan University takes a critical first step towards understanding the neuromuscular mechanisms behind DCD. Her primary aim was to expose children with DCD to different types of tasks in order to measure the underlying neuromuscular deficits associated with their impaired movement abilities.
To do this, Dr. Esselaar chose tasks and exercises that relate to common motor control deficits in children with DCD. Then, using Trigno Galileo HDsEMG sensors, Dr. Esselaar’s team identified motor unit patterns in children with DCD and compared them to those of typically developing (TD) children.
Her research has revealed initial findings on how the brain and muscles communicate in children with DCD and how that differs from TD children.
A Look at the Neuromuscular Level
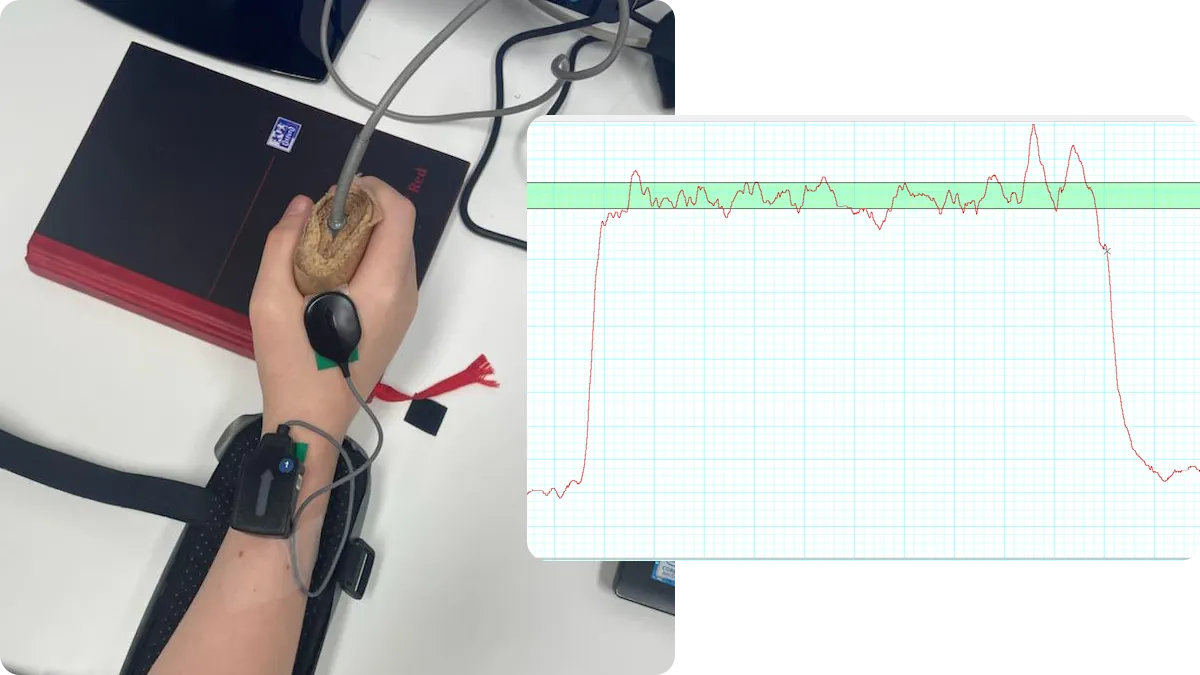
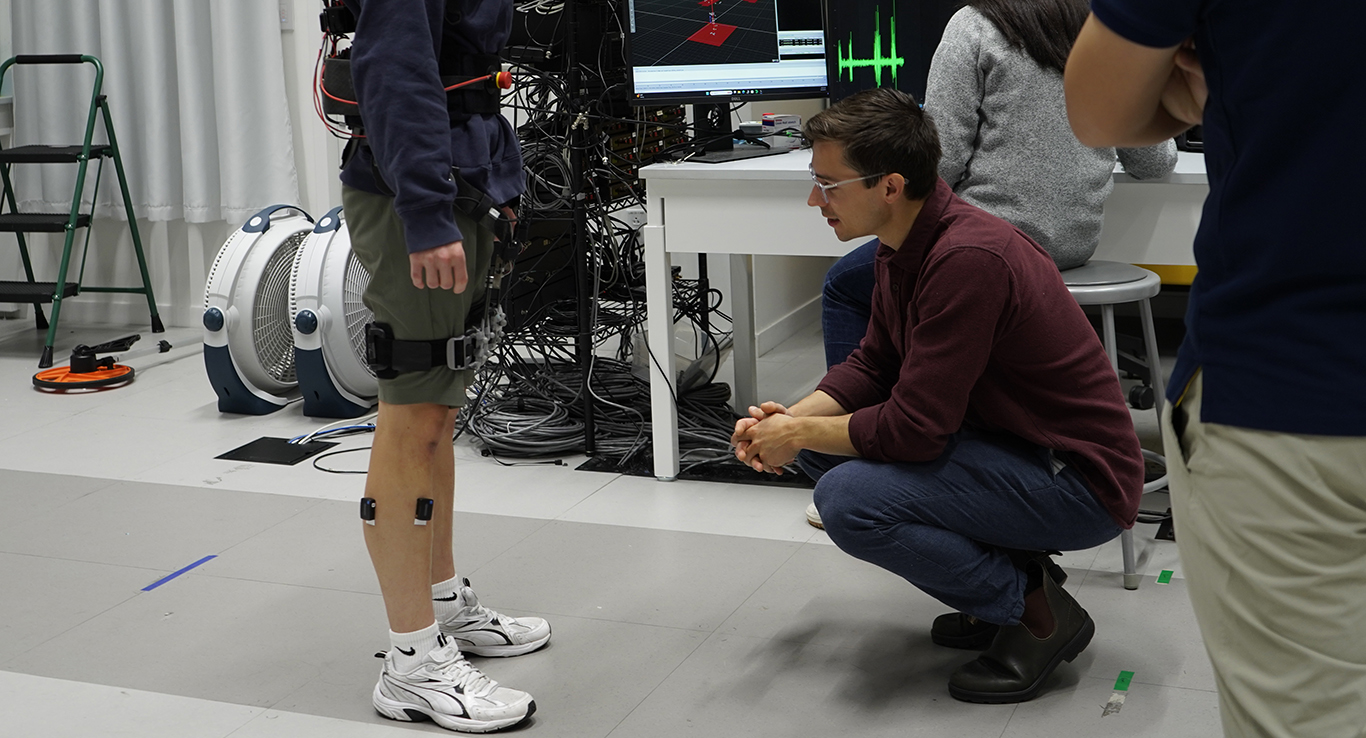
Figure 1: Trigno Galileo sensor placement and hand-held dynamometer (left) for a 10% MVC hold (right)
In this study, HDsEMG data was recorded from the first dorsal interosseus muscle during a hand-grip task. Force output was also recorded via a hand-held dynamometer that participants were asked to squeeze. This task was chosen because hand grip is associated with many actions that DCD children struggle to perform, including tying shoes, buttoning shirts, and other dexterous tasks.
Participants were instructed to contract 6 times at 10% of their maximum voluntary contraction (MVC), alternating between bursts of contraction and relaxation. In total, there were 11 trials per participant, yielding 66 individual bursts of muscle activity to examine.
Once data was collected, it was decomposed within the Neuromap software, where motor unit information was extracted and then compared between the DCD and TD groups. The researchers filtered the data for trials where force accuracy was high and variability was low. This was done to ensure that task performance was similar between the groups so that comparisons would reveal neuromuscular differences as opposed to differences in behavior. As a note, most of the data from the younger DCD children was excluded from the analysis, since it didn’t have enough accuracy and stability throughout the trials.
Results
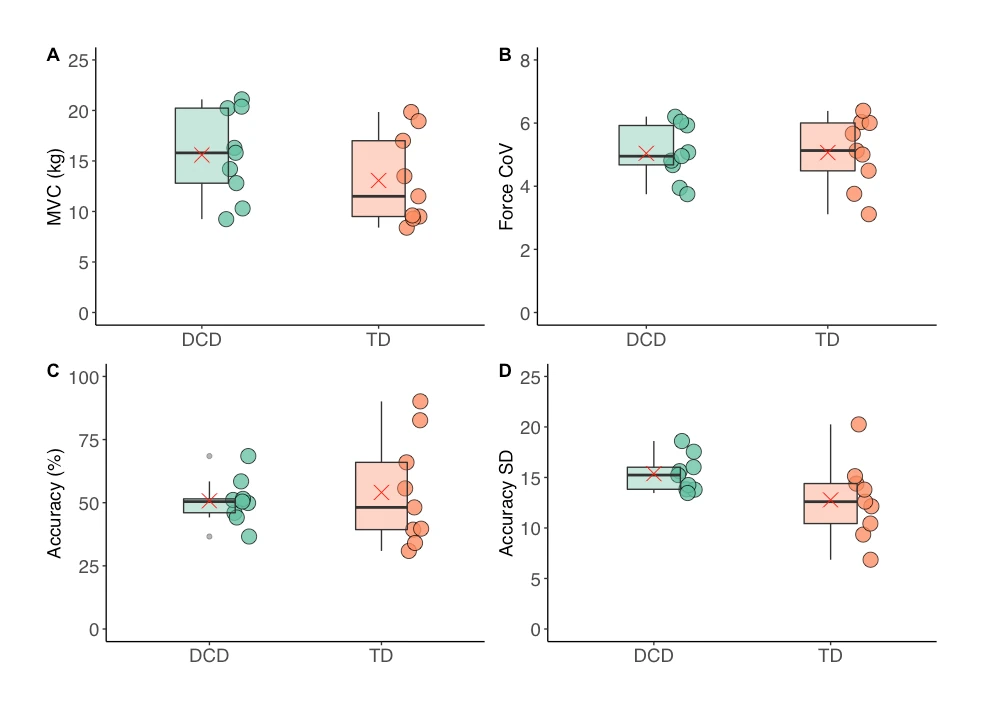
Since force data was used to ensure that task performance was similar between groups, there were no statistical differences in MVC (Figure 2A), force variation (Figure 2B), or force accuracy (Figure 2C) between the DCD and TD groups.
Figure 2: Box and whisker plots of (A) MVC, (B) force variation, (C) force accuracy, and (D) accuracy standard deviation in children with DCD vs. TD children.
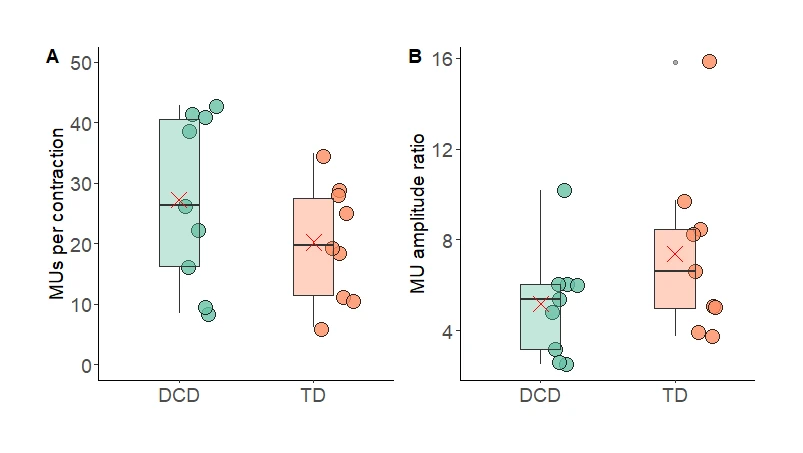
Additionally, the number of motor units (Figure 3A) and the motor unit firing rates (Figure 4A) were statistically similar between both groups, suggesting that the ability to recruit motor units may not be the primary mechanism disrupted by DCD. However, despite consistency in force production and motor unit firing rate, a deeper look at the motor unit data revealed some stark differences between the groups.
Figure 3: Box and whisker plots of (A) motor units per contraction and (B) motor unit ratio between small and large motor units in children with DCD vs. TD children.
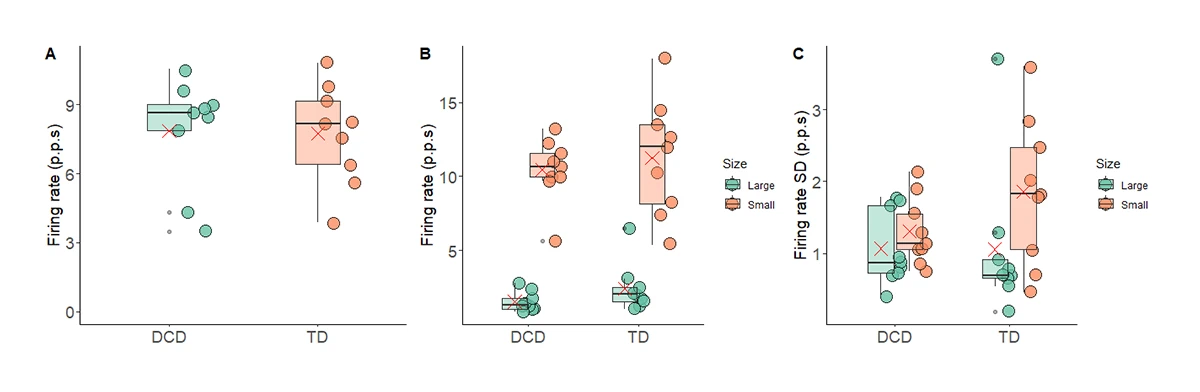
The firing rate standard deviation (FR-SD) of small motor units was significantly different to the FR-SD of large motor units in TD children (Figure 4C). Data from children with DCD did not show the same trend, with the FR-SD of small and large motor units having more uniformity.
Figure 4: Box and whisker plots of (A) motor unit firing rate, (B) firing rate of small and large motor units, and (C) firing rate standard deviation of small and large motor units in children with DCD vs. TD children.
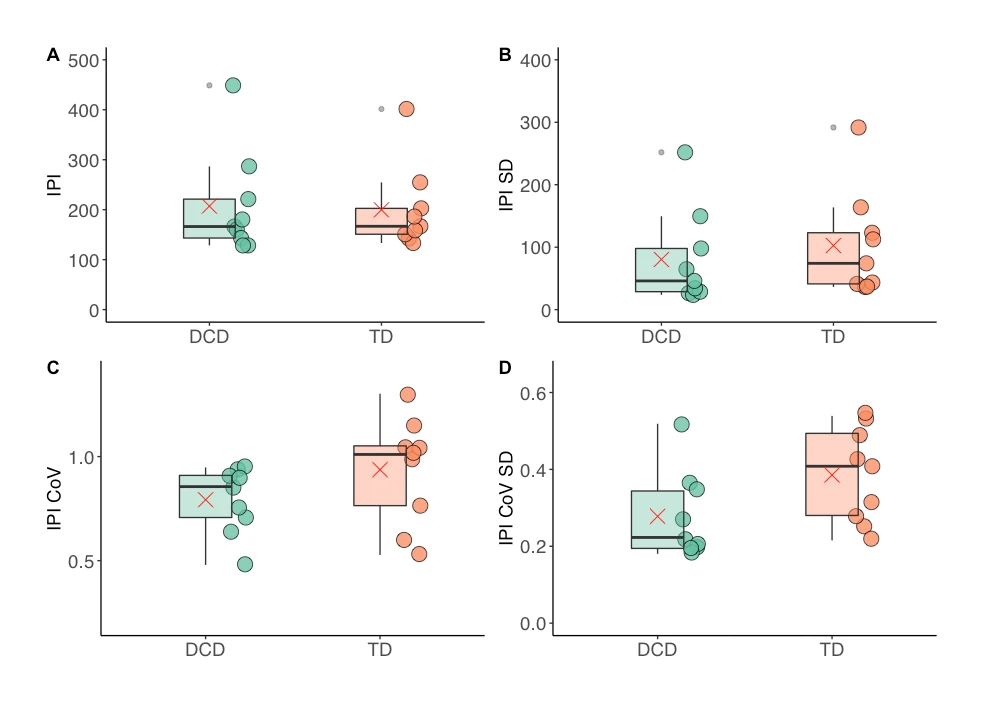
To a similar effect, the standard deviation of inter-pulse-interval variance (IPI-CoV-SD) was significantly greater in TD children, once again suggesting more uniformity in the motor unit activation patterns of children with DCD (Figure 5D).
Figure 5: Box and whisker plots of (A) inter-pulse-interval, (B) inter-pulse-interval standard deviation, (C) inter-pulse-interval variance, and (D) standard deviation of inter-pulse-interval variance in children with DCD vs. TD children.
Discussion
This study compares the neuromuscular patterns between DCD and TD children when task performance is held constant.
On the surface, both groups demonstrated a similar number of motor units and motor unit firing rates. However, further analysis of the FR-SD and the IPI-CoV-SD indicate that children with DCD performed the task with more fixed neuromuscular strategies. In other words, children with DCD seem to have less adaptable motor unit patterns than their TD counterparts. The patterns identified in FR-SD and IPI-CoV-SD also serve as useful biomarkers for DCD.
In the context of DCD, these findings are intuitive; it makes sense that a fixed neuromuscular system may have trouble adapting to new challenges. This could perhaps help explain why motor learning is such a difficult challenge for children with DCD.
Impact and Future Research
This research is the first of many steps to understanding the neuromuscular etiology of DCD. In the future, the neuromuscular biomarkers uncovered in this research may be useful in classifying the severity of DCD or in providing clinical biofeedback.
For Dr. Esselaar, she hopes to use these findings to assess and develop new therapies for children with DCD. Going forward, DCD therapies can be evaluated from a neuromuscular perspective, offering key insights into their efficacy.
HDsEMG offers a unique perspective on how neuromuscular tasks are achieved and helps to reveal hidden information about diseases and disorders. Dr. Esselaar is applying this concept to a new research focus: pedal error in drivers with diabetic peripheral neuropathy. She hopes to find a similar underlying neuromuscular biomarker to try and identify individuals who are at risk of pedal error before accidents occur.
Want to learn more about HDsEMG solutions offered by Delsys?
Children with developmental coordination disorder have less variable motor unit firing rate characteristics across contractions compared to typically developing children
Maaike Esselaar, Johnny V V Parr, Greg Wood, Emma Hodson-Tole
Overview and characteristics of DCD
Explore More Topics
Client Spotlight
Using HDsEMG to Uncover Neuromuscular Biomarkers in Children with Developmental Coordination Disorder (DCD)